
Imagine waking up and feeling like a shadow of your former self. You're exhausted despite eight hours of sleep, your gym gains have vanished, and your drive in the bedroom has completely disappeared. For millions of men, this isn't just "getting older"-it's a medical condition called male hypogonadism is a condition where the body doesn't produce enough testosterone, either due to a problem with the testes or the glands that control them. While it can feel isolating, it's a treatable endocrine disorder that affects roughly 4 to 5 million men in the U.S. alone.
Is it actually low testosterone?
Not every dip in energy is a hormone deficiency. To know if you're dealing with hypogonadism, you have to look at the specific physiological markers. Most men experience a mix of physical and mental shifts. One of the most telling signs is a drop in sexual health; about 85% of patients report a decreased libido, and nearly 80% notice fewer spontaneous erections. You might also see a physical transformation: a 20-30% loss in lean muscle mass and a 10-15% increase in body fat, even if your diet hasn't changed.
It goes deeper than just muscles and sex drive. Long-term deficiency can lead to osteoporosis in about 33% of affected men, with bone density dropping by 2-3% every year. Some men also experience mild anemia, as hemoglobin levels can dip below 13.5 g/dL. If you're noticing these patterns, it's time to stop guessing and get a blood test.
The two faces of hypogonadism
Not all low testosterone is created equal. Doctors split the condition into two main types based on where the "breakdown" is happening in your system.
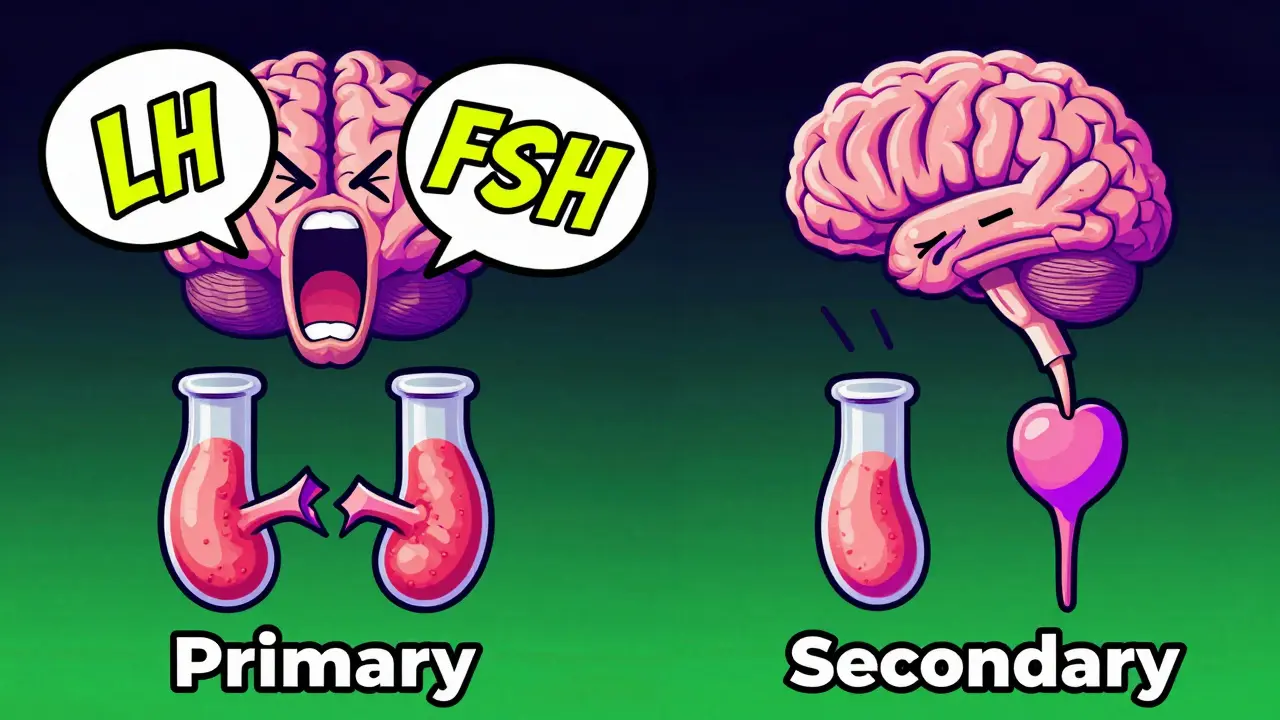
First, there's primary hypogonadism is testicular failure where the testes cannot produce testosterone despite signals from the brain. In this version, your brain is screaming at the testes to work by pumping out high levels of Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH). Common causes include Klinefelter syndrome (a genetic XXY pattern) or damage from mumps orchitis.
Then there's secondary hypogonadism is a failure of the hypothalamus or pituitary gland to signal the testes to produce testosterone. This is much more common, making up 85-90% of cases. Often, this is triggered by obesity, pituitary tumors, or chronic opioid use. Interestingly, for those whose low T is driven by weight gain, losing just 10% of body weight can boost testosterone levels by 30-40% without any medication.
| Feature | Primary Hypogonadism | Secondary Hypogonadism |
|---|---|---|
| Origin of Problem | Testes | Pituitary/Hypothalamus |
| LH & FSH Levels | High (>10 mIU/mL) | Low or "Inappropriately" Normal |
| Prevalence | 10-15% of cases | 85-90% of cases |
| Common Cause | Genetic/Injury (e.g., Klinefelter) | Obesity, Opioids, Tumors |
Getting a real diagnosis
You can't rely on a single random blood test. Testosterone follows a circadian rhythm, peaking between 8:00 AM and 11:00 AM. Because of this, the Endocrine Society recommends that diagnostic tests be done early in the morning. A diagnosis typically requires two separate morning measurements showing serum levels below 300 ng/dL.
The method of testing also matters. Mass spectrometry is the gold standard. Older immunoassay methods are prone to errors, showing 15-20% higher false-positive rates. If your levels are borderline (between 250-350 ng/dL), your doctor might order a free testosterone test using equilibrium dialysis to see how much hormone is actually available for your body to use.
Exploring therapy options
Once a deficiency is confirmed, Testosterone Replacement Therapy (TRT) is the medical administration of testosterone to return serum levels to a physiological range. The goal isn't to make you a bodybuilder, but to get you into the optimal range of 350-700 ng/dL to relieve symptoms.
There are several ways to deliver the hormone, and the "best" one depends on your lifestyle:
- Gels: Applied daily to the skin. They offer steady levels but carry a risk of transferring the hormone to partners or children through touch.
- Injections: Usually given every 2-4 weeks. They are cost-effective ($30-50/month) but can cause "peaks and troughs" where you feel great for a week and then crash.
- Pellets: Small implants inserted under the skin every 3-6 months. They provide the most stable levels but require a minor surgical procedure.
- Oral Capsules: Newer options like Jatenzo provide high bioavailability without the skin-transfer risks of gels.
The risks: What you need to watch out for
TRT isn't a vitamin; it's a powerful hormone with potential side effects. Some men experience acne or a thickening of the blood (polycythemia), which may require therapeutic phlebotomy (drawing blood to lower hematocrit). There is also the risk of testicular atrophy, as the body stops producing its own testosterone when it's being supplied externally.
More importantly, TRT isn't for everyone. Men with prostate cancer, severe heart failure, or hematocrit levels above 50% should generally avoid it. There has been significant debate regarding cardiovascular risks. While the FDA issued a black box warning in 2015 after some studies showed a 30% increase in heart attacks for men over 65, other experts argue that when used correctly, TRT can actually reduce all-cause mortality.

Real-world results and expectations
What does life actually look like after starting therapy? For many, the change is dramatic. Data from patient communities shows that about 73% of men notice an energy boost within two weeks, and 68% see a return of morning erections within a month. If paired with resistance training, a significant number of men gain 20-30 lbs of muscle over six months.
However, it's not a magic pill. Only about 25-35% of men achieve complete symptom resolution. This tells us that low testosterone is often just one piece of the puzzle. Factors like depression, sleep apnea, and chronic stress can mimic low T symptoms, and treating the hormone won't fix those underlying issues.
How long does it take for TRT to work?
Energy and mood improvements often happen quickly, sometimes within 2 weeks. However, changes in muscle mass, bone density, and full restoration of sexual function typically take 3 to 6 months of consistent therapy.
Will TRT make me infertile?
Yes, standard TRT can suppress sperm production because the brain stops signaling the testes to produce both testosterone and sperm. If you are planning to have children, you should discuss alternatives like HCG or Clomid with your doctor.
Can I stop taking testosterone once my levels are normal?
It depends on the cause. Men with genetic conditions like Klinefelter syndrome usually need lifelong therapy. However, men with obesity-related hypogonadism who lose significant weight may find their natural levels return enough to discontinue TRT.
What is the best time to test my testosterone?
Testosterone levels are highest in the morning. You should have your blood drawn between 8:00 AM and 11:00 AM for the most accurate reading.
Are there natural ways to increase testosterone?
Weight loss is the most effective natural method for those with obesity, as a 10% reduction in body weight can significantly boost T levels. Heavy resistance training and improving sleep quality are also proven to help.
Next steps for management
If you suspect you have low T, your first move should be a consultation with an endocrinologist or urologist. Avoid "quick fix" clinics that promise TRT without rigorous testing. A proper path looks like this: two morning blood tests via mass spectrometry, a review of your PSA (prostate-specific antigen) levels, and a hematocrit check.
If you're overweight, try 3-6 months of aggressive lifestyle changes first. Focus on strength training and a high-protein diet. If the numbers are still low and your symptoms persist, discuss the delivery methods-gels, injections, or pellets-to find the one that fits your daily routine and budget.