
When people hear the term COPD, they often think of one thing: trouble breathing. But COPD isn’t a single disease. It’s a group of lung conditions, and two of the most common-chronic bronchitis and emphysema-work very differently in the body. Even though they often show up together, treating them the same way can make things worse. Knowing the difference isn’t just academic; it changes how you breathe, how you live, and what treatments actually work.
What Exactly Is Chronic Bronchitis?
Chronic bronchitis isn’t just a bad cough that won’t go away. It’s a specific diagnosis: a productive cough that lasts at least three months a year for two years in a row. That’s the official definition from the American Thoracic Society in 2023. The problem starts in the airways. The lining of the bronchi gets inflamed, and the mucus-producing glands swell up-sometimes growing 300 to 500% larger than normal. Instead of producing 10 to 100 milliliters of mucus a day like healthy lungs, these lungs churn out 100 to 200 mL. That’s about half a cup of thick, sticky mucus daily. This mucus doesn’t just sit there. It clogs the airways. Tiny hair-like structures called cilia, which normally sweep mucus out, get damaged by smoke or pollution. So instead of being cleared, mucus builds up. That’s why people with chronic bronchitis spend so much time coughing-not because they’re sick, but because their lungs are trying to clear what they can’t expel naturally. Many describe it as a daily ritual: 20 to 30 minutes of chest physiotherapy just to loosen the gunk. You’ll often hear this called the “blue bloater” phenotype. Why? Because low oxygen levels turn lips and fingertips blue (cyanosis), and fluid retention causes swelling in the legs. The body’s trying to compensate. The heart works harder to push blood through damaged lungs, leading to cor pulmonale-a form of heart strain. These patients often feel worse in winter, when cold air triggers more mucus and infections.What Exactly Is Emphysema?
Emphysema is a quiet destroyer. It doesn’t make you cough. It makes you gasp. Instead of attacking the airways, emphysema eats away at the alveoli-the tiny air sacs where oxygen enters your blood. Think of them like balloons. In a healthy lung, they’re small, elastic, and spring back when you breathe out. In emphysema, the walls break down. The balloons merge into giant, floppy sacs. This isn’t just about size-it’s about surface area. You lose 40 to 60% of the area where oxygen and carbon dioxide swap places. That’s why even walking a short distance can leave you breathless. People with emphysema often don’t produce much mucus. Their main complaint? Air hunger. They describe it as never getting enough air, no matter how hard they breathe. Their lungs can’t push air out efficiently because they’ve lost elastic recoil. That’s why they sit forward, purse their lips, and breathe slowly-techniques that help trap air and keep airways open longer. This is the “pink puffer” phenotype. Their skin stays pink because they hyperventilate to get enough oxygen-breathing fast and shallow, sometimes 25 to 30 times a minute. Their chest becomes barrel-shaped as lungs overinflate. They look thin because their bodies burn extra calories just to breathe. But their oxygen levels? Often still in the 92-95% range. That’s why they don’t turn blue-until it’s too late.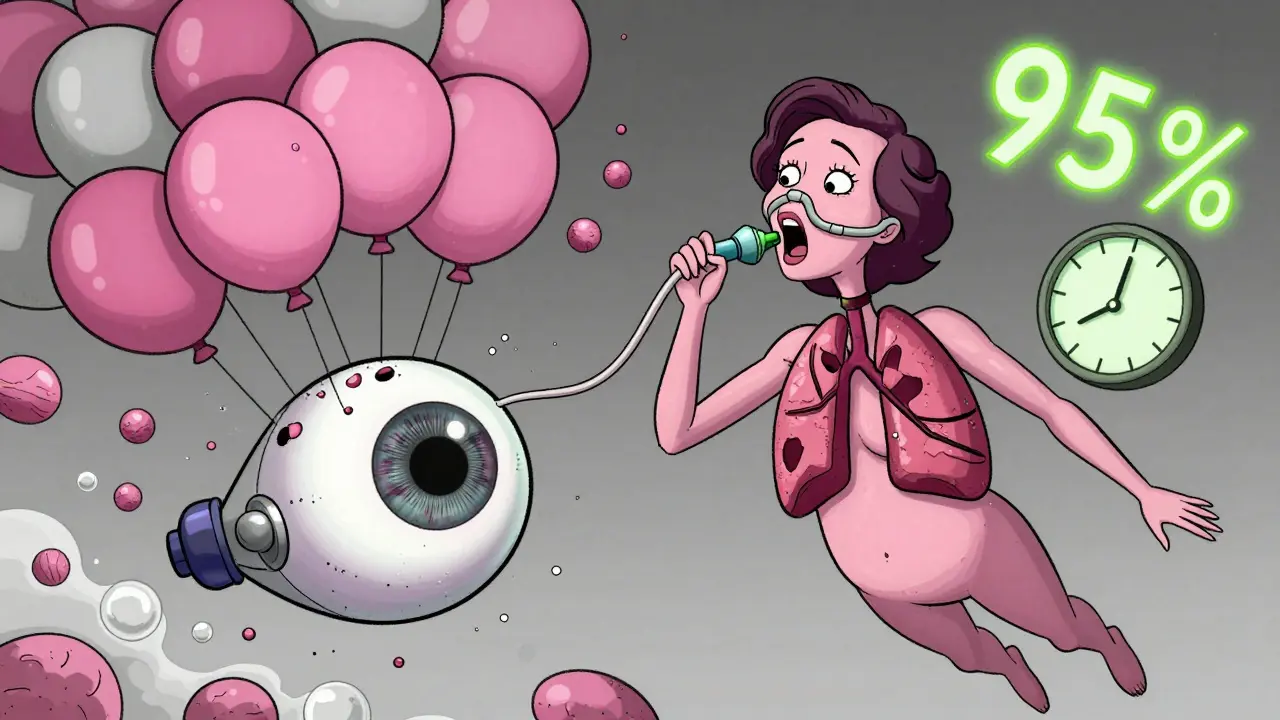
How Doctors Tell Them Apart
You can’t tell these two apart just by listening to someone cough. You need tests. The first step is spirometry: a simple breathing test that measures how much air you can force out in one second (FEV1) and how much you can exhale in total (FVC). In both conditions, the FEV1/FVC ratio drops below 70%. That confirms airflow obstruction-but not the cause. That’s where DLCO comes in. This test measures how well your lungs transfer carbon monoxide into your blood. It’s a direct readout of how much functional lung surface you have left. In emphysema, DLCO is usually below 60% of predicted. In chronic bronchitis? It’s often normal or only slightly lowered. If your DLCO is low, emphysema is likely playing a big role. CT scans show even more. In emphysema, you’ll see dark patches-areas where lung tissue has collapsed or disappeared. If more than 15% of the lung looks like that, it’s a clear sign. In chronic bronchitis, the CT shows thickened airway walls, especially on expiratory scans. The wall area percentage exceeds 60%, meaning the tubes themselves are swollen shut. The 6-minute walk test also gives clues. Emphysema patients usually drop their oxygen levels below 88% within two minutes. Chronic bronchitis patients don’t drop as much-they stop because they’re too out of breath, not because they’re running out of oxygen.Treatment Isn’t One-Size-Fits-All
This is where things get critical. Giving the same meds to both types can backfire. For chronic bronchitis, the goal is to thin and clear mucus. Mucolytics like carbocisteine reduce flare-ups by 22%. Hypertonic saline nebulizers help too-73% of users report thinner mucus. Inhaled steroids? Risky. Studies show chronic bronchitis patients have a 40% higher chance of pneumonia when using them. Instead, long-acting bronchodilators (LAMA/LABA combos) are first-line. If someone has more than two flare-ups a year, roflumilast-a pill that reduces inflammation-can cut exacerbations by 17.3%. Emphysema treatment focuses on saving lung function and improving airflow. Bronchodilators help, but they don’t fix the destroyed tissue. That’s why lung volume reduction surgery (LVRS) or endobronchial valves are options for severe cases. These procedures collapse the worst parts of the lung so the healthier parts can work better. In the 2021 IMPACT trial, patients improved their 6-minute walk distance by 35% after valve placement. For those with alpha-1 antitrypsin deficiency-a genetic form of emphysema-a weekly infusion of the missing protein can slow decline by 20%. Oxygen therapy helps both, but it’s often more life-changing for emphysema patients. Portable concentrators delivering 2-4 liters per minute can be bulky, and many report feeling trapped by the tubing. Still, for those with low oxygen, it’s the difference between staying home and being able to walk outside.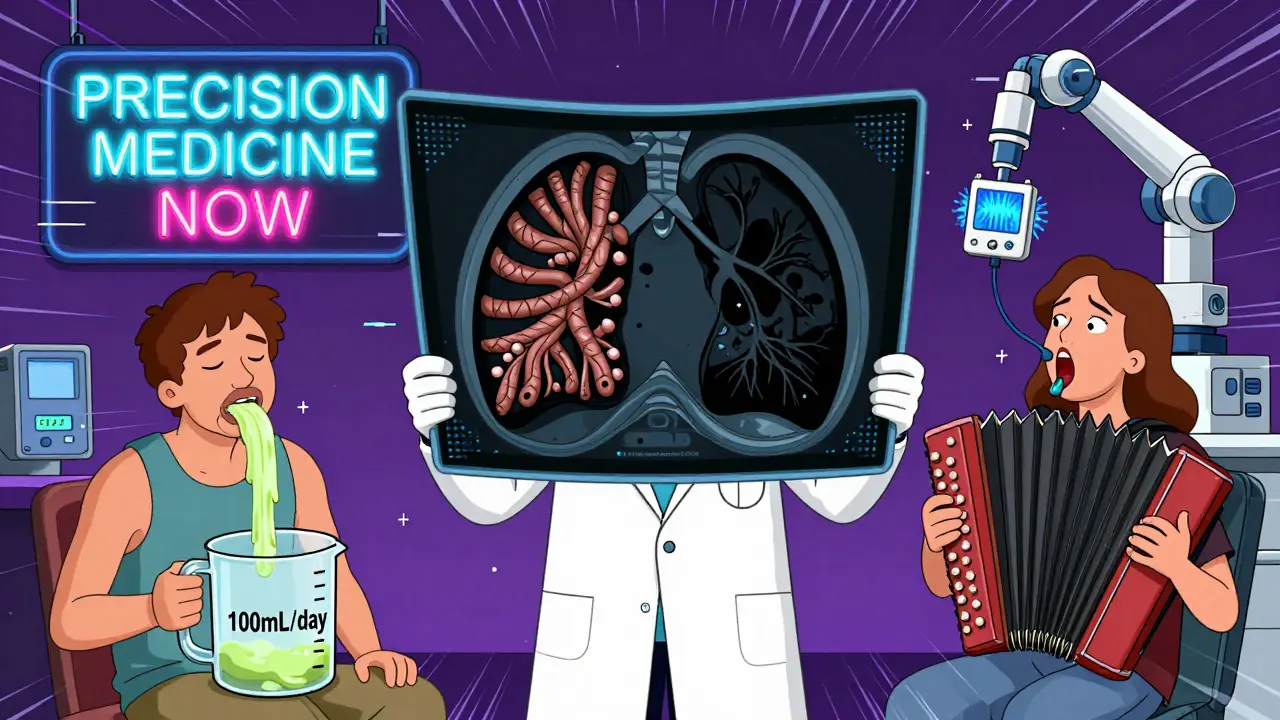
Real People, Real Lives
Patient stories reveal what the numbers don’t. One man on Reddit measured his morning mucus for eight years-100 mL every day, verified with a measuring cup. He did chest physiotherapy twice a day. He couldn’t travel far without a portable nebulizer. His life revolved around clearing his lungs. Another woman with emphysema said she could only speak five or six words before needing to stop and catch her breath. She stopped cooking, stopped gardening, stopped talking to friends on the phone. Her oxygen tank became her shadow. Both felt isolated. Both struggled with daily inhaler routines. Sixty-eight percent of chronic bronchitis patients in one study said taking four to six inhalers a day was overwhelming. Half of emphysema patients said oxygen therapy made them feel like prisoners in their own homes. But there’s hope. A 2022 European study found that hypertonic saline made mucus so much easier to clear that many patients cut their physio time in half. Another study showed endobronchial valves helped emphysema patients walk farther and breathe easier-without open surgery.Why This Matters More Than Ever
COPD is the fourth leading cause of death worldwide. In 2021, it killed 3.23 million people. And the numbers are rising. By 2030, prevalence is expected to jump 30%. The problem? Most doctors still treat COPD like one disease. But a 2022 study in the New England Journal of Medicine showed that when patients got treatment tailored to their specific type-bronchitis or emphysema-they had 27% fewer hospital visits. New drugs are coming. In 2023, the FDA approved an inhaled form of alpha-1 antitrypsin for genetic emphysema. In 2024, Europe launched a new acoustic device that vibrates mucus loose-no pills, no nebulizers. Researchers are now testing blood markers to predict who’ll respond to biologics. The message is clear: COPD isn’t one condition. It’s a mix of two very different diseases. And the future of treatment isn’t in more inhalers-it’s in precision medicine. Know which one you have. Ask for the right tests. Push for a personalized plan. Your lungs-and your life-depend on it.Can you have chronic bronchitis and emphysema at the same time?
Yes, and most people with advanced COPD do. While the terms "blue bloater" and "pink puffer" describe two main patterns, research shows only about 15% of severe COPD patients have pure forms of either condition. The rest have a mix-some airway inflammation, some alveolar damage. That’s why doctors now focus on the dominant features rather than trying to fit patients into one box.
Is COPD the same as asthma?
No. Asthma is usually reversible and often starts in childhood. People with asthma have airway spasms that respond well to inhalers and can go years without symptoms. COPD is progressive, usually starts after age 40, and is caused by long-term damage from smoking or pollution. The airflow blockage in COPD doesn’t fully reverse, even with treatment.
Does quitting smoking help if I already have COPD?
Absolutely. Even if your lungs are already damaged, quitting stops the damage from getting worse. Studies show people who quit after diagnosis slow their lung function decline by up to 50%. It also reduces flare-ups, lowers infection risk, and improves how well medications work. It’s the single most effective thing you can do.
Are there any new treatments on the horizon?
Yes. In 2023, the FDA approved an inhaled form of alpha-1 antitrypsin for genetic emphysema, showing a 20% improvement in lung function over a year. In 2024, a new acoustic device that shakes mucus loose without drugs launched in Europe, cutting exacerbations by 32%. Researchers are also testing biologics for chronic bronchitis patients with high blood eosinophils, and bronchoscopic thermal vapor ablation is showing 78% success in reducing emphysema damage over two years.
How do I know if I have chronic bronchitis or emphysema?
Start with a spirometry test. If your FEV1/FVC is low, ask your doctor for a DLCO test. A low DLCO suggests emphysema. If you have a long-term productive cough with frequent winter flare-ups, chronic bronchitis is likely. A high-resolution CT scan can confirm structural changes. Don’t assume-you need the right tests to get the right treatment.
Comments
srishti Jain
December 30, 2025 AT 23:22This post is overkill. I just wanted to know if my cough is bronchitis or if I’m dying. Now I have to learn DLCO and CT scans. Thanks.
Shae Chapman
December 31, 2025 AT 16:40OMG I cried reading the part about the woman who could only say 5 words before gasping 😭 My grandma had emphysema and she used to hold her oxygen tank like it was her baby. She’d whisper, ‘I just wanna feel the wind again.’ This post got it right. Thank you for writing this.
Aayush Khandelwal
December 31, 2025 AT 21:29The phenotypic dichotomy of COPD-blue bloaters versus pink puffers-is a clinically elegant heuristic, but it’s increasingly outdated in the era of mixed phenotypes. The 2022 NEJM study you cited confirms that heterogeneity trumps binary classification. The real paradigm shift lies in biomarker-guided stratification: blood eosinophils for bronchitic inflammation, alpha-1 antitrypsin levels for emphysematous destruction, and now, emerging proteomic signatures for exacerbation risk. We’re moving from anatomical descriptors to molecular endotypes. The future isn’t just precision medicine-it’s predictive, preemptive, and personalized.
Sandeep Mishra
January 2, 2026 AT 08:09It’s funny how we label people by their symptoms-blue bloater, pink puffer-as if their whole identity is their lungs. But behind every diagnosis is someone who used to hike, cook, laugh loud, or hold their grandkids. I’ve seen patients who stopped speaking on the phone because breathing took all their energy. That’s not just a disease. That’s a slow theft of life. And yet, we still treat COPD like it’s a broken pipe you can fix with a new valve. Maybe the real treatment isn’t in the lungs… it’s in how we see the person inside them.
Hayley Ash
January 3, 2026 AT 07:08So you're telling me I need a CT scan and a DLCO test just to know if I'm breathing wrong? And you think this is helpful? Newsflash: most people don't have access to these tests and your 'precision medicine' is just a fancy way to make doctors charge more. Also 'pink puffer'? That's not a diagnosis, that's a meme. Next you'll be calling asthma 'the wheezy waltz'
kelly tracy
January 3, 2026 AT 19:14Wow. Another feel-good article pretending to be science. You think people with COPD don’t know they’re sick? They’ve been told to quit smoking for 20 years. The real problem is the system that lets Big Pharma sell inhalers for $500 a month while ignoring pollution, industrial toxins, and lack of access to care. You’re not helping. You’re distracting. And no, I don’t need a 6-minute walk test to know I’m tired of being told to ‘breathe better’.
Kelly Gerrard
January 5, 2026 AT 03:30It is imperative to acknowledge that smoking cessation remains the single most efficacious intervention in the management of chronic obstructive pulmonary disease. The data are unequivocal. Continued exposure to tobacco smoke is the primary driver of disease progression. Therefore, it is incumbent upon all patients to prioritize abstinence. All other therapies are adjunctive.
Glendon Cone
January 6, 2026 AT 04:50Man, this hit different. I’ve got a buddy who’s been on oxygen for 5 years. He says the worst part isn’t the breathlessness-it’s the way people stare at his tank like it’s a monster. He says he feels like a walking medical device. This post? It didn’t just explain COPD. It showed the people behind the stats. And that acoustic device in Europe? That’s the kind of innovation that actually gives back freedom. Props to the researchers. And to everyone still breathing through the fog-you’re not alone.